 |
| His arms clamp around my throat. I fight
with all my might, but within ten seconds the ringing in my ears
becomes deafening. The dojo spins; it seems to be more of a fuzzing
out. Then, total blackness. |
 |
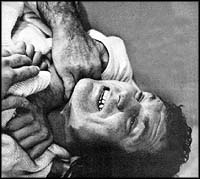
HADAK - JIME (BARE ARM CHOKE)
 This is one of the
easiest and fastest chokes to apply. As mentioned in the article,
this choke can cause extreme pain. Since these findings were first
,published, revisions in the applica tion of the choke have been
intro. duced making them more effective. Applying the choke, the
attacker brings his right arm around the op ponent's neck, slipping
it underneath the chin of the victim. The radius bone of the
attacker's arm must be wedged against the carotid artery. The
attacker must keep his head tight against his opponent, forcing the
victim to hunch-over and bend into himself. This is one of the
easiest and fastest chokes to apply. As mentioned in the article,
this choke can cause extreme pain. Since these findings were first
,published, revisions in the applica tion of the choke have been
intro. duced making them more effective. Applying the choke, the
attacker brings his right arm around the op ponent's neck, slipping
it underneath the chin of the victim. The radius bone of the
attacker's arm must be wedged against the carotid artery. The
attacker must keep his head tight against his opponent, forcing the
victim to hunch-over and bend into himself.
| It takes only a moment to realize
I am on the mat, face down. I am certain only a half-second has passed,
but my opponent is waiting in the center of the fighting area, his judo gi
neatly refolded and black belt re-tied.. He's staring the confident glare
of the victor. From the looks of things I must have been out for at least
half a minute, possibly more.
My teammates later
report he knocked me out for the full count plus 20. It's hard to believe
because I had jumped up, ready to defend myself, and felt prepared to
continue the battle. But the match was over. "Ippon!" was called.. I lost.
How many judoka
have experienced the same choke-out and unconsciousness? The first time,
it's a spooky feeling - the not -quite - knowing -for - sure. Is it any
wonder parents and physicians are among those most vehemently opposed to
judo's use of the choke hold?
It seems to be the not
knowing that is the main objection to choking or what is referred to by
judoists as shimewaza. It was precisely this lack of knowledge that
prompted the Kodokan to scientifically and intensively study the effects
of choking the human body. A description of the experiments and the
accompanying results were published by the Kodokan in a bilingual
(Japanese and English) book called the Bulletin of the Association for the
Scientific Studies on Judo, Kodokan, Report 1, "Physiological Studies on
Choking in Judo."
Is there any danger in
the use of shimewaza? This is what a team of experts came together to try
to discover. Representing several of Japan's foremost medical schools and
universities as well as the Kodokan, this group of medical specialists and
ranking educators used the electroencephalograph to detect brain changes;
the earoxymeter for blood oxygen saturation, the sphygmomanometer for
arterial blood pressure; the plethysmograph peripheral blood vessel
reaction and the micropipometer for skin temperature changes. Other
studies probed the plasma protein concentration, blood water volume,
hematrocrit complete blood count, eosinophil count and urine 17
keto-steroid content.
Scientific Search for Danger
Three other objectives
to the study were to discover the differences in the effect of the various
choking methods, the duration of the effect of choking on the body, and
the physiological mechanism of the resulting state of unconsciousness.
Three methods of choking were used: okurieri-jime, the neck squeezed as a
whole; katajuji-jime, the carotid arteries' region pressed; hadaka-jime,
the trachea depressed.
 |
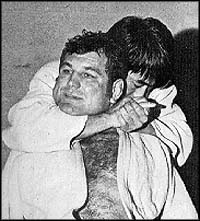
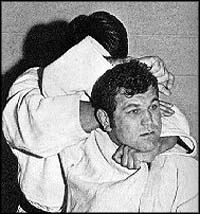
KATAJUJI - JIME (ARM CROSS CHOKE)
One of the most
commonly used chokes in competition is the katajujijime and, yet, it
seems to be-the most difficult to apply. The attacker begins the
choke by facing his opponent and grasping the lapel with his left.
Crossing the left and grabbing the opponent's right lapel with his
right hand, the attacker inserts his thumb deep into the jacket and
grasps a tight reign on the lapel. The opponent's lapel is used as a
rope and is cinched tight across the opponent's left carotid artery
while the attacker's right arm is jammed into the right side of the
opponent's neck. |
 |
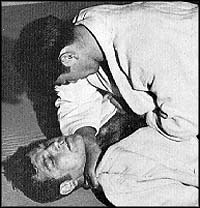
OKURIERI - JIME (DEEP LAPEL CHOKE)
Grabbing the
opponent by the lapel with the left hand, and wedging the bare arm
under the chin, this choke is applied by the attacker from the rear.
As the opponent moves his right arm up to break the hold of the
attacker's left hand on his lapel the attacker comes from underneath
the right arm-pit with his right, slipping between the shoulder and
the nape of the neck, forcing the opponent's right arm up in the air
and exerting pressure on the neck.
|
Describing the technique
of choking in the 1968 AAU-USJF Official Judo Handbook, Dr. E. K. Kiowai
explains, "Basically, except for one form of shimewaza, hadaka-jime the
pressure is applied to the lateral side of the neck which the anatomists
call the 'carotid triangle' . . . In the center of this triangle are the
jugular veins, carotid artery and its branches and the carotid sinus. No
strong muscle protects this area. The pressure is applied in a certain
manner, depending upon the technique, directly on these structures. It may
be the fist or the collar of the judogi. Very often it is the pressure of
the dista end (joint) of the radius and the wrist which compresses the
soft structures of the neck. Until the above name structures
are-'sufficiently compressed the choke will not be effective. The neophyte
may submit not because of the choke but because of the fear of being
choked or the pain produced by improper choking methods." As Dr. Koiwai
explains it, the hadaka-jimi choke hold is dif ferent from other forms
because part of the pressure is applied to the larynx and trachea which is
extremely painful and the player will usually submit before
unconsciousness intervenes.
Short of submission, be
will fight all the harder for the release because of the excruciating pain
accompanied by this hold.
Six high-ranking black
belt judoists were used for the Kodokan experiment. Five of the black
belters were used as victims while the last, a sixth dan, performed the
choking using the three, above-mentioned methods. Only in the
katajuji-jime were the subjects strangled from the front. The victims were
laid on a couch in the resting position, looking as though they were wired
for sound. The other two forms of choking were performed while the upper
part of the victims' bodies were raised approximately 30 degrees and the
performer did the strangulation from behind.
As all the-equipment was
checked and re-checked, the experiment was given the okay to commence. The
sixth dan who was to perform the choking took his position and was given
the signal to go ahead. The criteria for unconsciousness was the reflex
dilation, or widening, of the pupils. The choker released his hold at the
first sign of unconsciousness. Measurement on the eyes' pupils were made
at rest, then at the ready position, and finally throughout the choking
period until five minutes after regaining consciousness. The three chokes
were performed on each of the five subjects so a total of 18 tests were
recorded and analyzed. Some of the general symptoms the subjects elicited
were interesting to the novice as well as the seasoned judoka.
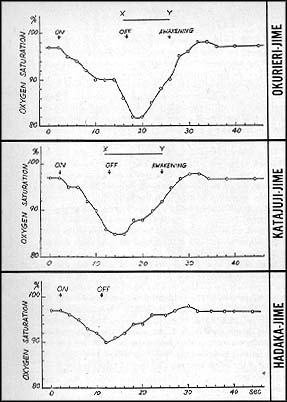 |
EFFECT ON OXYGEN SATURATION
Measuring the
percentage of oxygen saturation in the blood of the helix of the ear
with an earoxymeter, the top two choke holds show a marked drop in
the amount of oxygen being absorbed while bottom graph shows only a
slight decline. |
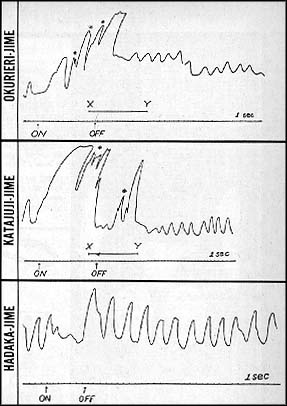 |
EFFECTS ON RESPIRATION
Convulsions are
noted only on the top two charts by a "*" while it is noted on the
hadaka-jime choke hold the subject had no convulsions and maintains
conscious throughout. |
After only 10 seconds of
choking, the victims fell unconscious. As soon as they were diagnosed
unconscious, the per former released them and, the subjects remained
unconscious from 10 to 12 seconds. During this period the victims some
times developed clonic, a jerking or fluttering, cramps. All subjects woke
up spontaneously. It was mentioned in the Bulletin the victims sometimes
bad dreams which were "not unpleasant" while they were unconscious. After
awakening, the subjects did not complain of any unpleasant feelings.
It seems the
pain threshhold on the hadaka-jime method of choking was too great to
induce unconsciousness and would be a poor method to rely on in tournament
play because the opponent would probably fight all the more to gain
release. However with the okurieri-jime and the katajuji-jime all the
subjects lost consciousness and entered a state that was similar in many
respects to that of sleeping. As the subject regained consciousness
spontaneously his electroencephalogram readings returned to normal. It
should be repeated that in all the cases the performer released his grip
immediately after the subjects fell unconscious, thereby limiting the
effect of choking to a short period. But had the strangulation continued
serious aftereffects would have been expected.
What causes
unconsciousness from choking? The findings show the stopping of the flow
of blood to the bead plays an important role in causing the
unconsciousness. In other words-, the subject blacks out due to the lack
of oxygen in the brain which is fed blood via the carotid arteries.
Notes Epileptic Seizure
Also linked to this lack
of oxygen to the brain are the convulsions which sometimes accompany the
judo choke knockout. The electroencephalograph recorded symptoms very
similar to that of a short epileptic seizure.
To prevent any dangers
that may accompany the choke, the Kodokan bulletin advises it is dangerous
to perform the choking bold on subjects with cardiac disorders or those
suffering from hypertension since the load to the heart and the rise in
blood pressure is marked. It is also advised that it is dangerous for
youngsters whose nervous system and heart have not yet attained complete
development.
|